The Six Steps: How Babies are Born
Labor is the process by which a woman gives birth to a baby and the placenta. Surprisingly there are a lot of steps involved in a baby coming into the world. Our bodies work hard to make this happen. In the short sense, here’s what happens when a woman gives birth:
Contractions of her uterus, the largest and strongest muscle in the woman’s body.
Softening (ripening), thinning (effacement), and opening (dilation) of her cervix.
Breaking of her bag of waters (the membranes of amniotic sac) that surrounds the baby, and the release of her water (amniotic fluid).
Rotation of her baby and the molding of the baby’s head to fit into the mother’s pelvis.
Descent of the baby out of the uterus and through the birth canal (vagina) to the outside.
Birth of the placenta.
Trouble is, there’s only one part of labor most of us (especially our peanut galleries) seem to focus on: progress. And what do most of us base progress on? Dilation of course! Turns out, labor progresses in six ways and that’s the major takeaway here. Labor progress is measured by more than just dilation, just as birth is measured by more than just pushing a baby out.
LABOR PROGRESSES IN SIX WAYS
The cervix softens (or ripens). While still thick, the cervix, through the action of hormones and prostaglandins, softens and becomes more pliable.
The position of the cervix changes. The cervix points toward your back during most of pregnancy, then gradually moves forward. The position of the cervix is assessed by a vaginal exam and is described as posterior (pointing toward the back), midline, or anterior (pointing toward the front).
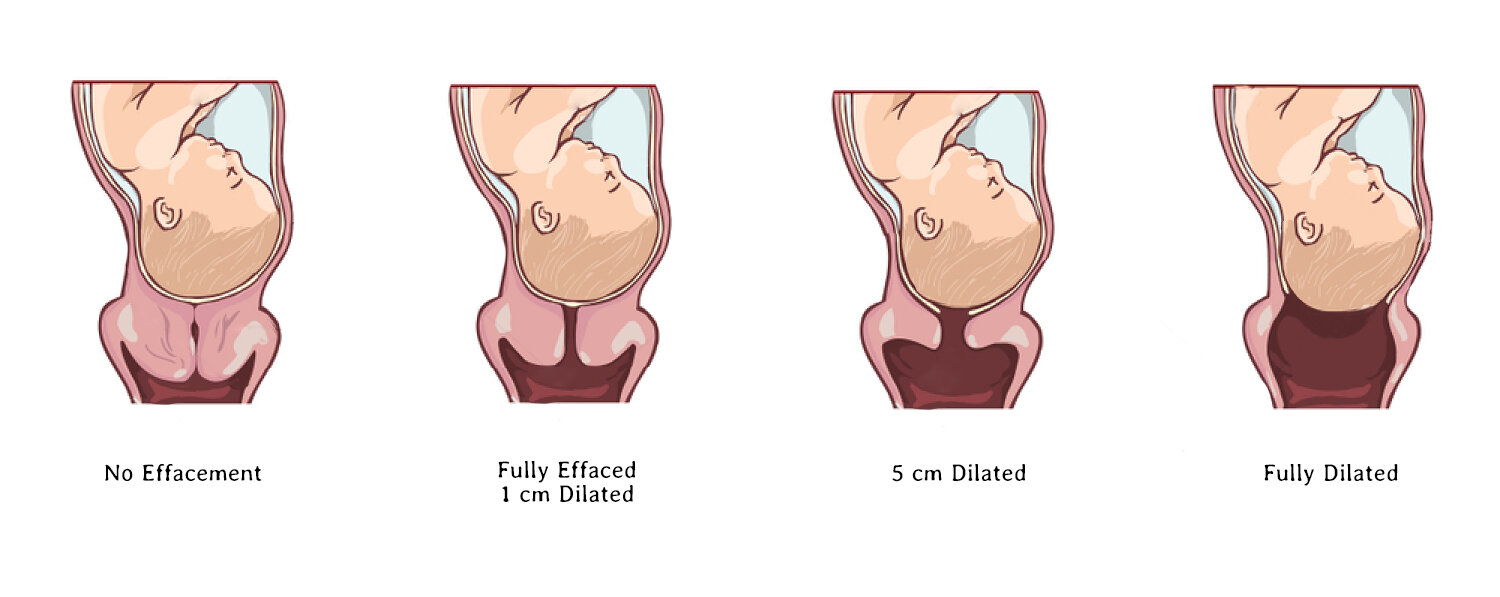
The cervix thins and shortens (effaces). Usually about 1 and 1/2 inches (or 3 to 4 cm) long, the cervix gradually shortens and becomes paper-thin. The amount of thinning (effacement) is measure in two ways: percentages and centimeter of length. Most often, you will hear health providers refer in percentages. 0% means no thinning or shortening has occurred; 50% means the cervix is about half it’s former thickness; 100% means it is paper-thin.
The cervix opens (dilates). The opening (dilation) of the cervix is also measured in centimeters. Dilation usually occurs with progressing contractions, after the cervix has undergone the changes described above. It’s common for the cervix to dilate 1 to 3 cm before there are noticeable signs of labor. Dilating before onset of labor is never an indication of when labor is likely to occur or how quickly progression will happen.
The baby’s chin tucks onto his chest (flexion) and his head rotates. The rotation makes it easier for the baby to pass through the birth canal. Sometimes, especially if the head is large, it must mold before it can rotate. This means that the head changes shape, becoming longer and thinner. Molding is normal, although some babies’ heads look somewhat misshapen for a day or two following the birth, after which time the head returns to a round shape. The most favorable position for birth is usually when the back of baby’s head (occiput) points toward your front or belly (anterior). This position is called OA.
The baby descends. The head continues to mold as necessary to fit and descend through the cervix, the pelvis and the vagina to the outside. The descent is described in terms of station, which (A) tells how far above or below your mid-pelvis the baby’s head is; (B) is measured in centimeters; and (C) ranges from -4 to +4. A zero station means the baby’s head is right at your mid-pelvis . Negative numbers mean baby’s head is above mid-pelvis. Positive numbers mean the head is to the outside and being born (crowning). Some descent occurs before labor and may be referred to as baby engaging into the pelvis.
Now putting it all together— here’s the MOST IMPORTANT thing to remember. Steps 4 through 6 (dilation beyond 2 to 3 centimeters, rotation, and descent) cannot take place until the first three steps are well underway. In other words, a cervix that is firm, thick or posterior WILL. NOT. OPEN. It is simply not ready. And a baby won’t rotate and descend significantly until the cervix is open. For some women, these changes happen quickly. For others, these changes take place gradually over several weeks at the end of pregnancy. There is no right or wrong way for these first steps to occur.
Dilation is important because it’s a measurable factor that we can easily understand and connect with as parents. The opening has to open completely, and then we have a baby. Check. Got it. But dilation is nothing to get hung up on. Birth is a multifaceted communication system between your baby and your body and ultimately, focusing on just how many centimeters dilated you are can lead to a lot of frustration on timing or what we perceive should be the timeline we birth in.
I encourage all families in birth to remember… there are so many things happening here. So instead of saying “am I dilated” at your 39 week appointment, if you prefer to be checked maybe ask instead, “How thin am I?” “Is my cervix still high up?” Dilation will occur when all of the other factors are met and it’s never reliable as a predictor of when a baby will arrive. While early progress is encouraging, it is not a requirement to have a baby without an induction or without other medical interventions.